


Methods of aerosol extraction in the dental clinic: a comparison
How to control infective aerosols created during examination and treatment processes is a challenge dental staff have always faced. Dental personnel and patients are exposed to tens of thousands of aerosols containing bacteria and viruses per cubic meter, and the potential to breathe contaminated air is high [1]. COVID-19 has heightened the concern about aerosols in the dental office.
While it is common practice for staff to wear PPE, this only mitigates some of the risks of transmission and it is known that this does not provide total protection to its wearer. More can be done to stop aerosols reaching surfaces, equipment, and the breathing zone of the dental staff and it is recommended that the risk could be further reduced by diverting, capturing, and containing it within a suitable extraction and filtration device where it can become no longer viable and then disposed of in a safe manner.
Good extraction can have a very definite positive impact on the spread of infection, reducing the amount of aerosol transmitted during dental procedures. The marketplace is full of systems that state they offer adequate protection and claims of effectiveness can be grossly misleading. Knowing what to purchase for a proper infection control regime can be confusing, and costly if the right choices aren’t made – financial and to the health of dental staff. This document considers the options available.
What additional interventions are best?
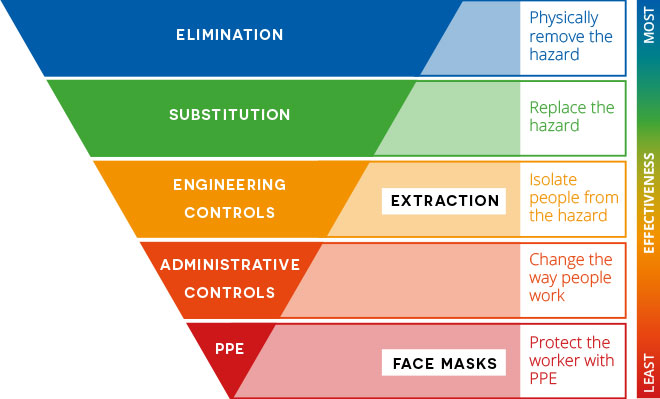
The hierarchy of control tool is used widely across industries to minimize exposure to hazards.
Use of an extractor is an example of protection through use of an engineering control. Use of extraction systems with high grade HEPA filters can provide an added (and in some cases higher) level of protection. These types of controls generally take time to produce and implement so administrative controls (some may be temporary) and PPE may be appropriate supplements as they are quick to implement, until more effective controls can be put in place [2].
A comparison of options
Viruses such as COVID-19 spreads primarily through droplets of saliva or discharge from the nose when an infected person coughs or sneezes, or via the aerosols created during examination and procedure [3]. Within a dental clinic, aerosols can remain in the air for a long time, may be transported for long distances in airflows and can contaminate areas beyond the patient’s immediate vicinity [4]. Furthermore, risk is present when airborne droplets settle on surfaces. There is also evidence that some microorganisms live within splash or spatter and even when the surface dries, they may become airborne as dust particles [5].
An effective system needs to remove air pollutants created in the dental surgery. Extraction in place direct at the patient’s mouth gives the best chance of capturing the contaminate at source.
Direct extraction, also known as local exhaust ventilation (LEV), is a method of hazard control where a nozzle generating an airflow is placed at the source of a contaminant in order to capture it and then pass it through filters.
In the context of a dental surgery, where the patient’s mouth is the potential source of bacteria or virus, a nozzle would be placed next to their mouth to capture aerosol generated by dental procedures. When used in conjunction with other protective measures, such as PPE, this can act as the first line of defense and even overcome some of the shortcomings of PPE.
Direct extraction is the only method that ensures the maximum possible level of aerosol capture.

All other methods listed below have greater risk of virus or bacteria landing on the clinical team.
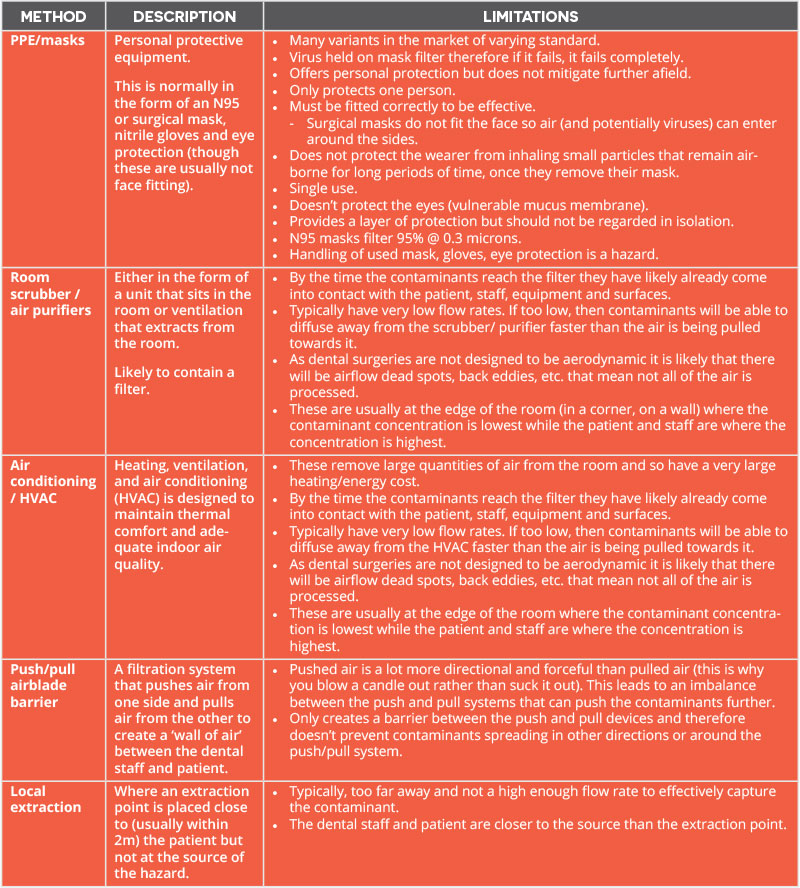
Although providing a level of protection, none offer the level of protection necessary to the immediate clinical team that direct extraction provides:

DIRECT aerosol extraction is the only effective method.

BOFA has the answer
DentalPRO Aerosol- maximum protection, minimal interference
The DentalPRO Aerosol helps to reduce risk of cross contamination between dental staff and the patient during examination.
With a market leading airflow to ensure optimum capture, it is designed to work alongside appropriate PPE guidelines. The DentalPRO Aerosol works by extracting contaminated air away from dental staff breathing zones and passing through a series of filters.
It is simple to use and maintain, and there’s no need to vent outside as the filtered air is sent back into the room. Its three-stage filtration includes a HEPA filter which removes 99.997% of particles at 0.3 microns.
The unit works on three set points: idle mode, AGP mode, and room scrubber mode.
Due to the large adjustable flow rate, the DentalPRO Aerosol may be used for a variety of procedures between dental staff and patient and can be turned to maximum capacity for applications that involve heavier aerosol generation.

• Fully portable and easy to move into position
• Supplied with multi-joint arm and funnel capture device making
this a versatile unit
• Low noise level, so won’t interrupt clinician-patient interaction
• Movable arms allow the inlet nozzles to be positioned in multiple locations to suit the requirement
• Detachable nozzles and inlets for easy change and cleaning
• Three-stage filtration
‣ DeepPleat pre-filter to remove larger particulate including dust associated with solidified paste in many dental processes
‣ HEPA filter to remove 99.997% of particles at 0.3 microns
‣ Odour/gas filter
• Ergonomically designed
• High airflow and high vacuum for maximum aerosol capture
• Variable speed – adjust as required
• Easy to operate
• Filter condition indicator
• Multi-voltage sensor automatically adjusts to local voltage (90-257V)
• Powerful pump, serviceable for 20,000+ hours
• Three set points: idle mode, AGP mode, and room scrubber mode
• British made and CE marked
Capture – Control – Filter
1. https://decisionsindentistry.com/article/transmission-precautions-for-dental-aerosols/
2. https://www.assp.org/news-and-articles/2020/03/31/how-to-apply-the-hierarchy-of-controls-in-a-pandemic
3. https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations
4. https://www.dentalcare.com/en-us/professional-education/ce-courses/ce619/airborne-droplets
5. https://www.dentalcare.com/en-us/professional-education/ce-courses/ce619/airborne-droplets